Cranial nerve lesions , part 4 (Vestibulocochlear nerve) скачать в хорошем качестве
Cranial nerve lesions , part 4 (Vestibulocochlear nerve)
1 месяц назад
Не удается загрузить Youtube-плеер. Проверьте блокировку Youtube в вашей сети.
Повторяем попытку...
Повторяем попытку...
Скачать видео с ютуб по ссылке или смотреть без блокировок на сайте: Cranial nerve lesions , part 4 (Vestibulocochlear nerve) в качестве 4k
У нас вы можете посмотреть бесплатно Cranial nerve lesions , part 4 (Vestibulocochlear nerve) или скачать в максимальном доступном качестве, видео которое было загружено на ютуб. Для загрузки выберите вариант из формы ниже:
-
Информация по загрузке:
Скачать mp3 с ютуба отдельным файлом. Бесплатный рингтон Cranial nerve lesions , part 4 (Vestibulocochlear nerve) в формате MP3:
Если кнопки скачивания не
загрузились
НАЖМИТЕ ЗДЕСЬ или обновите страницу
Если возникают проблемы со скачиванием видео, пожалуйста напишите в поддержку по адресу внизу
страницы.
Спасибо за использование сервиса ClipSaver.ru
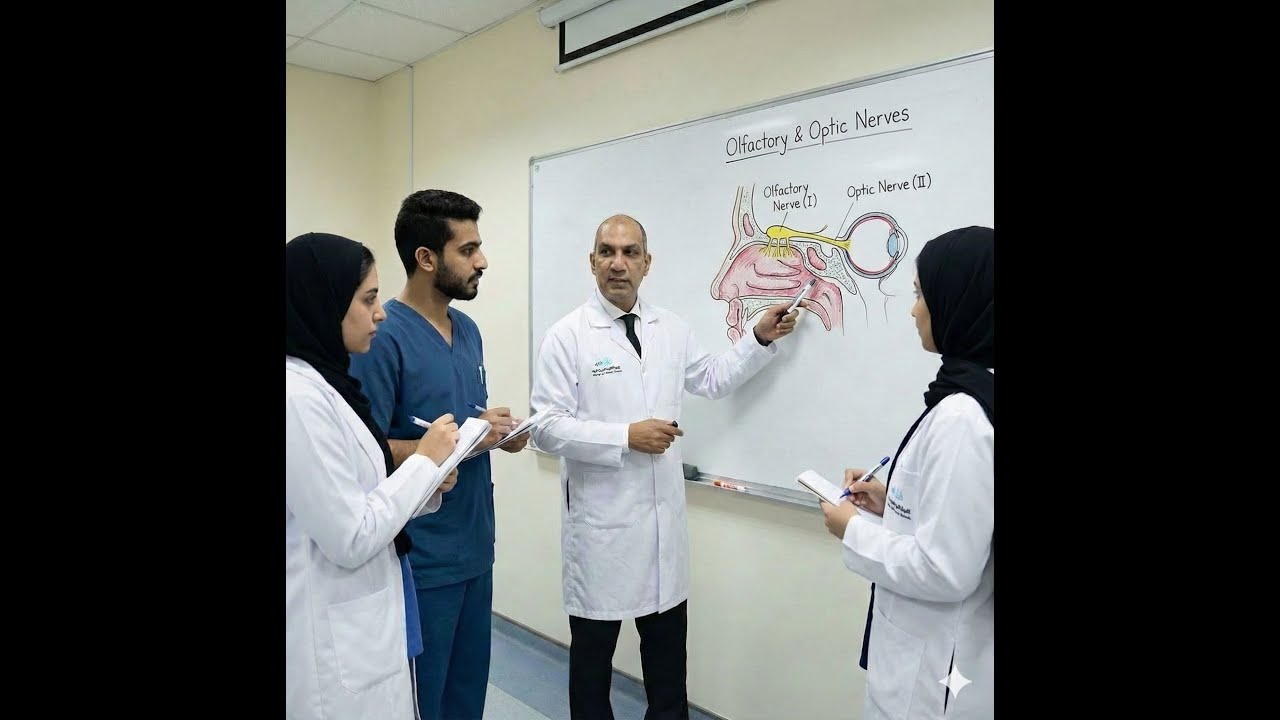
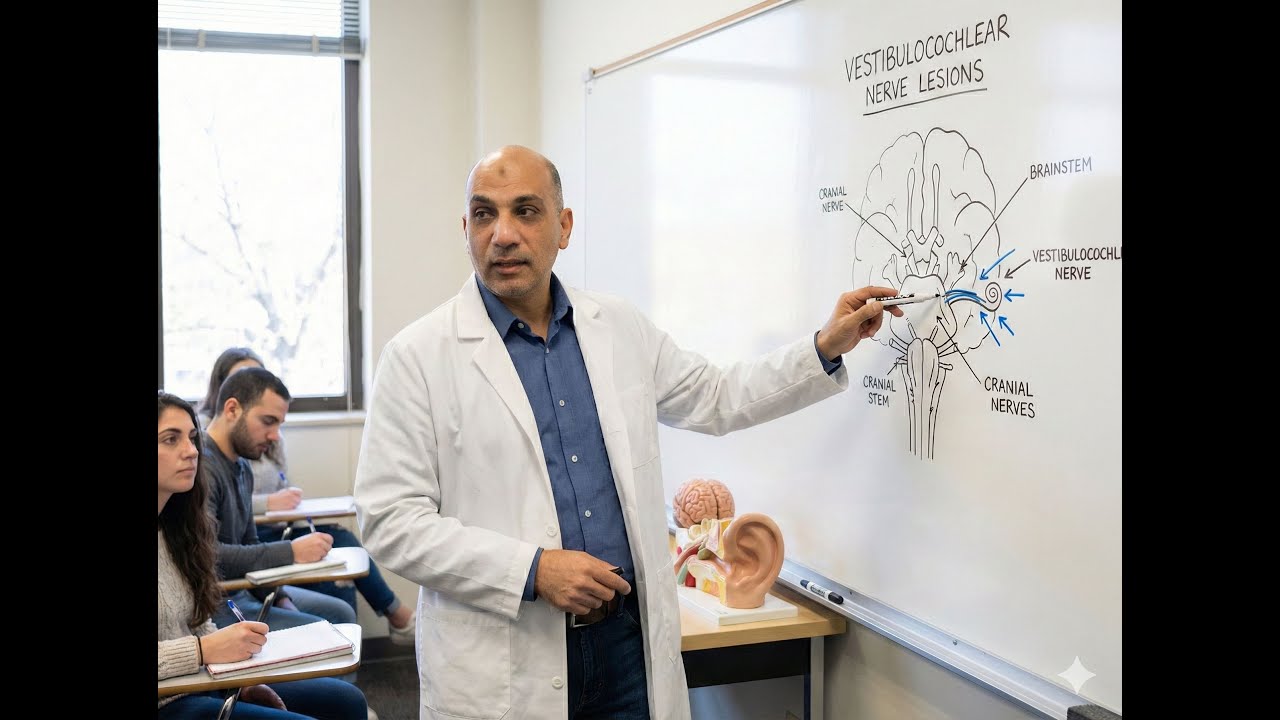
Cranial nerve lesions , part 4 (Vestibulocochlear nerve)
https://drive.google.com/file/d/1DC7U... Summary of Cranial Nerve VIII (Vestibulocochlear) Lesions The Vestibulocochlear Nerve (CN VIII) is a purely Special Somatic Afferent (SSA) nerve with dual functionality: an Auditory Component (transmits sound from the Organ of Corti) and a Vestibular Component (transmits proprioception for equilibrium/balance). I. Anatomy and First-Order Neurons: Cell bodies are bipolar neurons located in peripheral ganglia. Auditory Origin: Spiral Ganglion, housed in the modiolus of the cochlea. Vestibular Origin: Scarpa's Ganglion, located in the lateral end of the Internal Acoustic Meatus (IAM). CN VIII and the Facial Nerve (CN VII) travel together through the IAM. The IAM is divided into four quadrants: CN VII (Anterior Superior), Superior Vestibular Nerve (Posterior Superior), Cochlear Nerve (Anterior Inferior), and Inferior Vestibular Nerve (Posterior Inferior). The nerve enters the brainstem at the Pontomedullary Junction. II. Lesion Differentiation: Peripheral vs. Central | Feature | Peripheral (Nerve) | Central (Nuclei) | | :--- | :--- | :--- | | Location | CPA/IAM, nerve trunk | Brainstem (Pons/Medulla) | | Hearing Loss | Unilateral SNHL Common | Usually Normal (Auditory Sparing) | | Vertigo | Mild (chronic/tumor) due to compensation | Severe, persistent ("Central Storm") | | Nystagmus | Horizontal/Rotary, suppressed by fixation | Vertical or Direction-changing, NOT suppressed | | Key Etiology | Vestibular Schwannoma (Acoustic Neuroma) | Ischemic Stroke, Multiple Sclerosis | III. Central Vascular Syndromes AICA Syndrome (Lateral Pontine): Caused by occlusion of the Anterior Inferior Cerebellar Artery (AICA). High-Yield Triad: Vertigo, Ipsilateral Deafness (due to Labyrinthine Artery occlusion), and Ipsilateral Facial Weakness (CN VII). Mnemonic: Dizzy and Deaf (Face). PICA Syndrome (Lateral Medullary/Wallenberg): Caused by infarction of the Lateral Medulla. Key Distinction: Hearing is typically PRESERVED. Differentiator: Nucleus Ambiguus (CN IX, X) involvement, leading to Dysphagia (swallowing difficulty) and Hoarseness. Mnemonic: Dizzy and Hoarse (Throat).
Comments