Management of Hormone Receptor Positive Non-Metastatic Breast Cancer скачать в хорошем качестве
Management of Hormone Receptor Positive Non-Metastatic Breast Cancer
3 недели назад
Не удается загрузить Youtube-плеер. Проверьте блокировку Youtube в вашей сети.
Повторяем попытку...
Повторяем попытку...

Скачать видео с ютуб по ссылке или смотреть без блокировок на сайте: Management of Hormone Receptor Positive Non-Metastatic Breast Cancer в качестве 4k
У нас вы можете посмотреть бесплатно Management of Hormone Receptor Positive Non-Metastatic Breast Cancer или скачать в максимальном доступном качестве, видео которое было загружено на ютуб. Для загрузки выберите вариант из формы ниже:
-
Информация по загрузке:
Скачать mp3 с ютуба отдельным файлом. Бесплатный рингтон Management of Hormone Receptor Positive Non-Metastatic Breast Cancer в формате MP3:
Если кнопки скачивания не
загрузились
НАЖМИТЕ ЗДЕСЬ или обновите страницу
Если возникают проблемы со скачиванием видео, пожалуйста напишите в поддержку по адресу внизу
страницы.
Спасибо за использование сервиса ClipSaver.ru
Management of Hormone Receptor Positive Non-Metastatic Breast Cancer
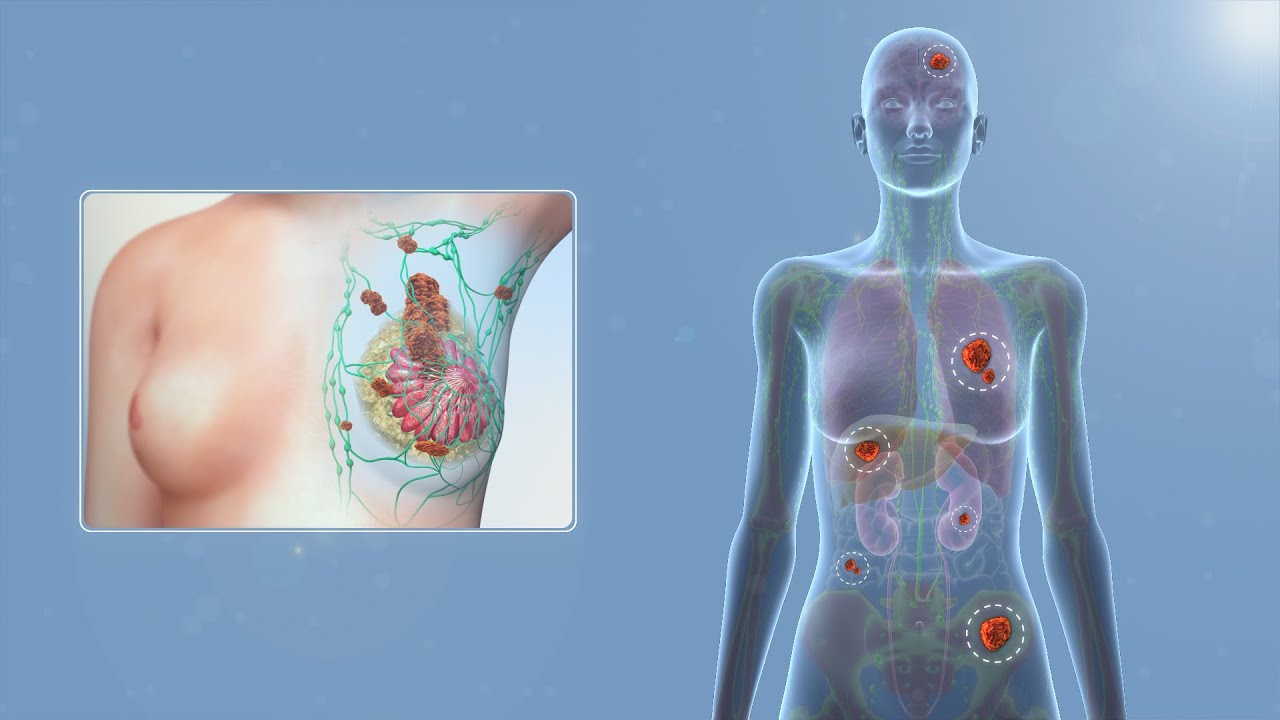
An in-depth overview of the management of HR positive Breast cancer including: 1] Breast Cancer Recurrence Genomic Prediction tools (eg. Oncotype Dx, Mammaprint) 2] Evolution of chemotherapy in Breast Cancer 3] Evolution of Endocrine therapy 4] Ovarian function suppression 5] CDK 4/6 inhibitors and other adjuvant agents Points to NOTE: 1) Rarely you can get ER-Neg, PR-Positive scenario. This is controversial and is considered by some experts to be an IHC staining artefact. Many physicians do give endocrine therapy in such scenarios. The addition of CDK 4/6i and other agents is however questionable. 2) For all premenopausal patients, adjuvant Tamoxifen for 10 years was the standard of care. Currently, in the presence of age less than 35 years, grade 3, indication for chemotherapy, or Tx size greater than 2cm, we also add Ovarian function suppression in the form of GnRh agonists (for 5 years as per SOFT/TEXT). This can be given as TAM x 10 yrs + OFS x 5 yrs OR as AI x 5 yrs + OFS x 5 yrs. When starting of with AI + OFS in a premenopausal patient, we have to regularly monitor FSH, Estradiol to ensure menopausal status. 3) In young women, another option for OFS is the ASTRA protocol where post surgery and chemotherapy you can monitor for re-occurrence of periods and S. FSH, S.estradiol 6 monthly for 2 years. If periods resume or S. FSH and estradiol return to premenopausal range, you can give OFS for 2 years. If this does not happen after 2 years of monitoring, the patient is considered to be in permanent menopause. 3) In post-menopausal women, AI x 5 years is the standard of care. We have data for prolonged AI to 7 and even 10 years. Prolonging more than 7 years has no survival benefit and leads to increased risk of fractures as per IDEA and SALSA trials. AI prolongation can be considered in patients with locally advanced breast cancer (T4/N2-3). 4) Amongst the adjuvant treatments, Hormone therapy can be started along with radiation, while CDK 4/6i and PARPi should be started after radiation There will be another session on indications for adjuvant radiation.
Comments