USMLE Renal 9: Anion Gap Explained (Acid Base, Graphs and More) скачать в хорошем качестве
USMLE Renal 9: Anion Gap Explained (Acid Base, Graphs and More)
8 лет назад
Не удается загрузить Youtube-плеер. Проверьте блокировку Youtube в вашей сети.
Повторяем попытку...
Повторяем попытку...

Скачать видео с ютуб по ссылке или смотреть без блокировок на сайте: USMLE Renal 9: Anion Gap Explained (Acid Base, Graphs and More) в качестве 4k
У нас вы можете посмотреть бесплатно USMLE Renal 9: Anion Gap Explained (Acid Base, Graphs and More) или скачать в максимальном доступном качестве, видео которое было загружено на ютуб. Для загрузки выберите вариант из формы ниже:
-
Информация по загрузке:
Скачать mp3 с ютуба отдельным файлом. Бесплатный рингтон USMLE Renal 9: Anion Gap Explained (Acid Base, Graphs and More) в формате MP3:
Если кнопки скачивания не
загрузились
НАЖМИТЕ ЗДЕСЬ или обновите страницу
Если возникают проблемы со скачиванием видео, пожалуйста напишите в поддержку по адресу внизу
страницы.
Спасибо за использование сервиса ClipSaver.ru
USMLE Renal 9: Anion Gap Explained (Acid Base, Graphs and More)
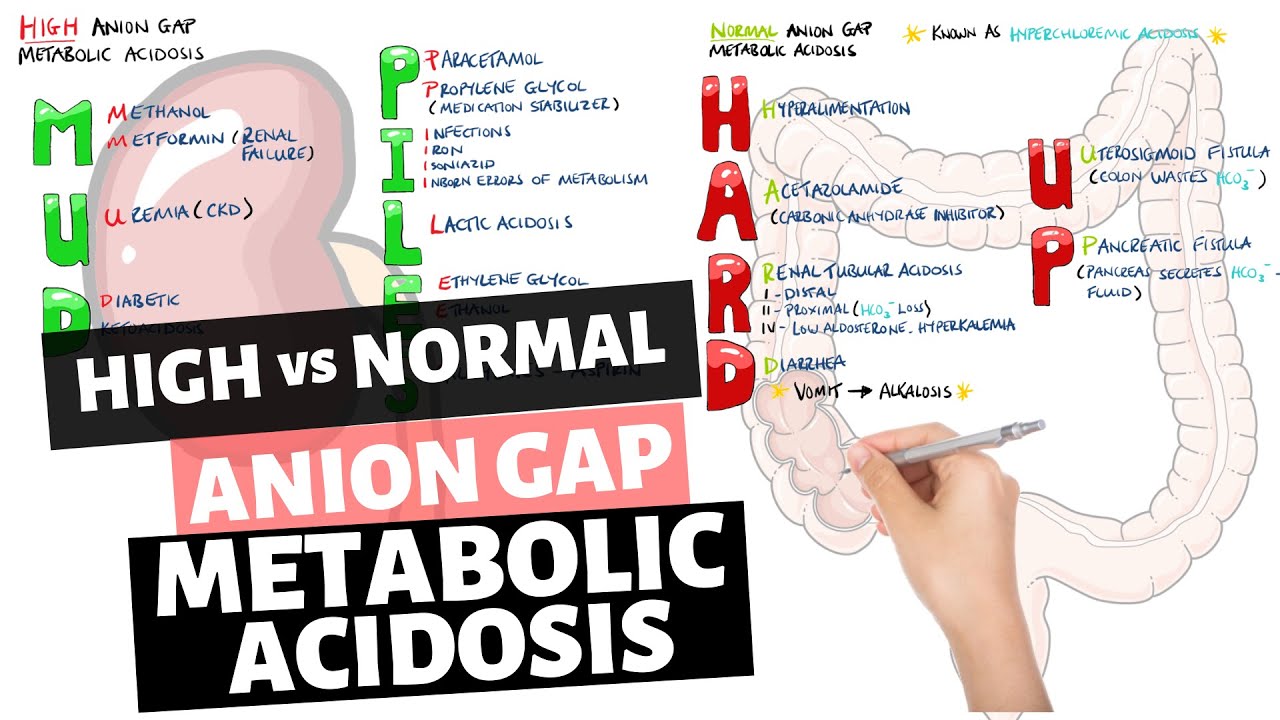
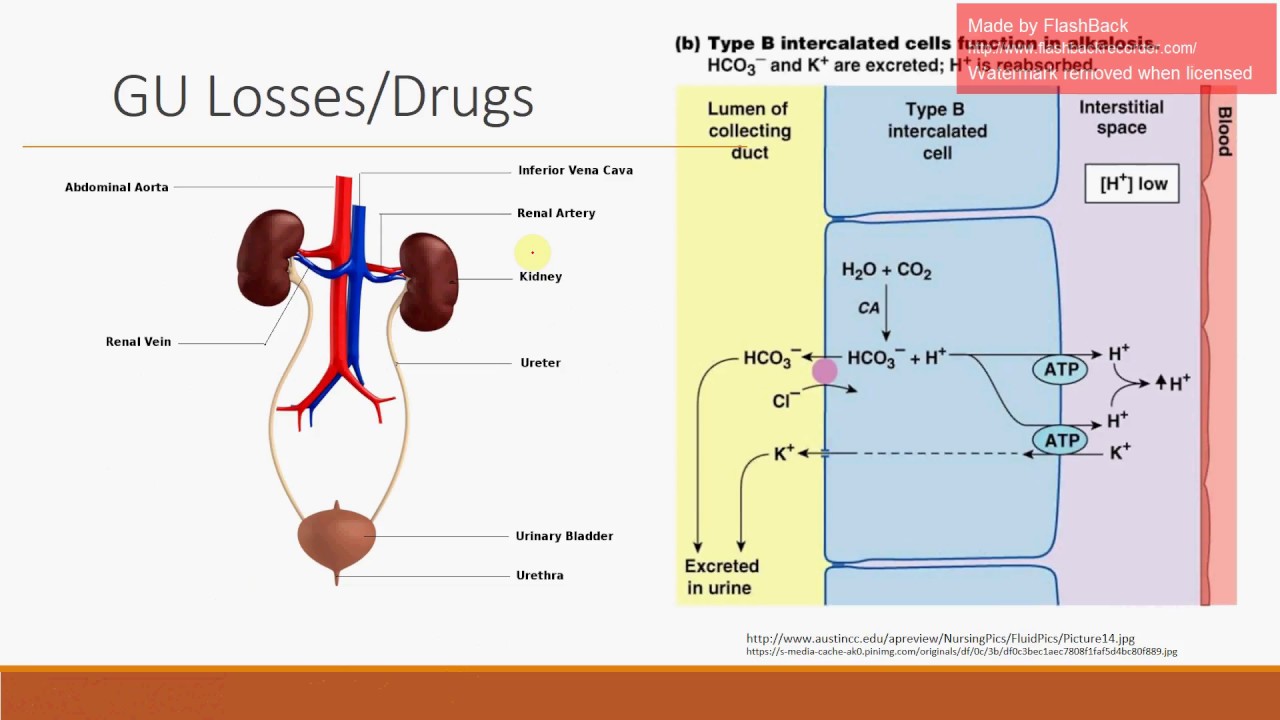
Want to support the channel? Be a patron at: / lymed Welcome to LY Med, where I go over everything you need to know for the USMLE STEP 1, with new videos every day. Follow along with First Aid, or with my notes which can be found here: https://www.dropbox.com/sh/mt1jrikc24... Thought you were done with renal physiology? Wrong! This next video is incredibly important and often tested on the boards. This is acid base homeostasis. Now you know your kidneys are very important in acid base control, as it helps move H+ and bicarb. Changes here are called metabolic acidosis or alkalosis. You should also know that your lungs are important in balance by controlling CO2. If you want to retain some acid, you hypoventilate. Conversely, if you want to lose acid you will hyperventilate. Changes here are called respiratory acidosis and alkalosis respectively. Some rules to keep in mind: your body likes homeostasis and will compensate if there is some sort of acidosis or alkalosis. However compensation is never complete and metabolic compensation takes a while. Now let's talk about some changes. Respiratory alkalosis: this occurs when you hyperventilate and you breathe out CO2. CO2 levels in labs will be low. Causes include hypoxemia, pulmonary embolus and early salicylate toxicity as it stimulates the respiratory center. Respiratory acidosis: this occurs in hypoventilation and retention of the acidic CO2. Causes include obstruction, opitate overdose, lung disease and neuromuscular pathologies. Metabolic alkalosis: this is due to loss of H+ or retention of bicarbonate. This can occur in vomiting and diarrhea, antacid use, diuretics especially loop diuretics via contraction alkalosis and hyperaldosteronism. Metabolic acidosis: this can be broken into anion gap and non-anion gap. What is the anion gap? Well in your body you have cations (like sodium and potassium) as well as anions like chloride and bicarbonate. Now your serum is neutral so you expect if you subtract anions from cations, it'll be zero. However it isn't! It's a positive number, meaning there is more cations than anions and this we call the anion gap. Why isn't it zero? Well because our equation doesn't account for some mystery anions/acids floating around. If you increase these acids than it increases your anion gap and causes anion gap acidosis. Causes of anion-gap acidosis include ingestion of formic acid, DKA, propylene and ethylene glycol (turns to oxalic acid), salicylate toxicity (late), lactic acidosis, iron overdose, isoniazid, and uremia (a result of metabolic acidosis). Non-anion gap acidosis: this is due to loss of bicarb and increased reabsorption of chloride to compensate. Causes include acetazolamide, renal tubular acidosis and hypoaldosteronism. We'll quickly talk about renal tubular acidosis here. You have several types. Type 2 works in your PCT and stops you from reabsorbing bicarb. Type 1 works on your alpha intercalated cell that stops excretion of H+, and type 4 is due to a failure of aldosterone. Our last topic will talk about common acid base charts and graphs they like to test you on.
Comments