Peripheral Neuroanatomy, Human Anatomy, USMLE Step 1 - Full Vignette with Extended Explanations скачать в хорошем качестве
Peripheral Neuroanatomy, Human Anatomy, USMLE Step 1 - Full Vignette with Extended Explanations
5 часов назад
Не удается загрузить Youtube-плеер. Проверьте блокировку Youtube в вашей сети.
Повторяем попытку...
Повторяем попытку...
Скачать видео с ютуб по ссылке или смотреть без блокировок на сайте: Peripheral Neuroanatomy, Human Anatomy, USMLE Step 1 - Full Vignette with Extended Explanations в качестве 4k
У нас вы можете посмотреть бесплатно Peripheral Neuroanatomy, Human Anatomy, USMLE Step 1 - Full Vignette with Extended Explanations или скачать в максимальном доступном качестве, видео которое было загружено на ютуб. Для загрузки выберите вариант из формы ниже:
-
Информация по загрузке:
Скачать mp3 с ютуба отдельным файлом. Бесплатный рингтон Peripheral Neuroanatomy, Human Anatomy, USMLE Step 1 - Full Vignette with Extended Explanations в формате MP3:
Если кнопки скачивания не
загрузились
НАЖМИТЕ ЗДЕСЬ или обновите страницу
Если возникают проблемы со скачиванием видео, пожалуйста напишите в поддержку по адресу внизу
страницы.
Спасибо за использование сервиса ClipSaver.ru
Peripheral Neuroanatomy, Human Anatomy, USMLE Step 1 - Full Vignette with Extended Explanations
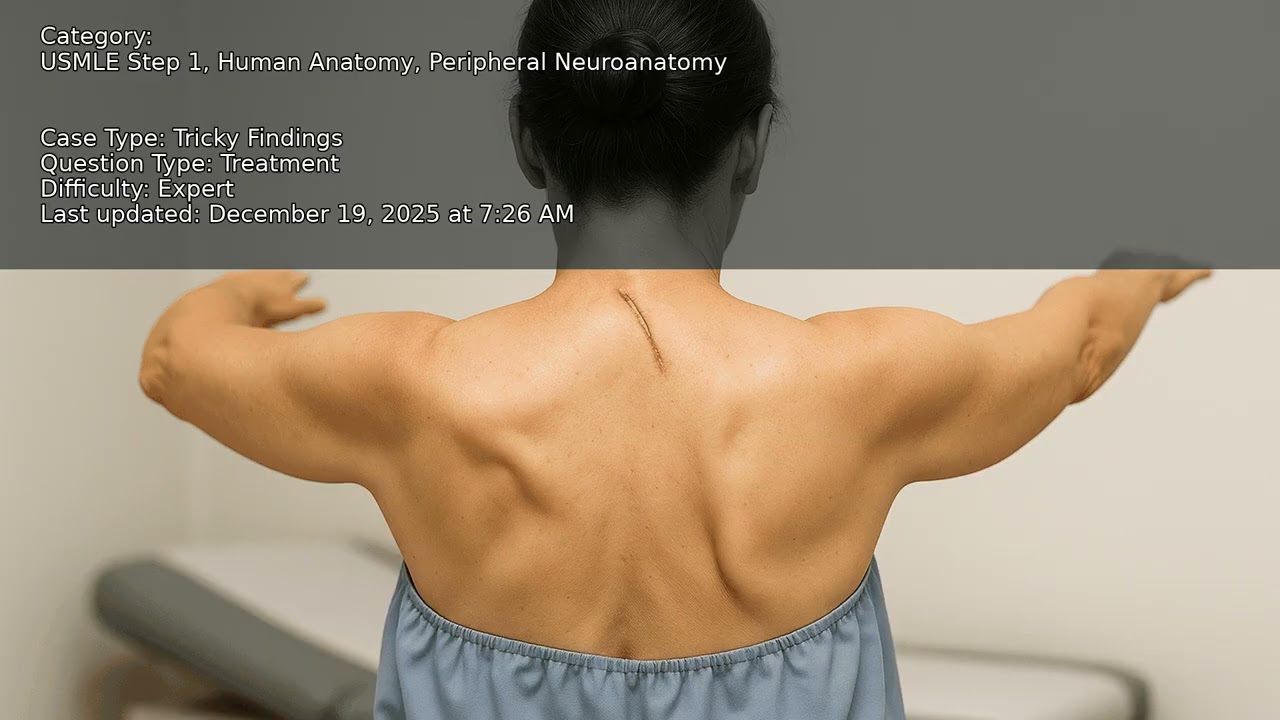
A 48-year-old woman develops new right shoulder girdle pain, prominent asymmetry, and weakness in arm abduction shortly after undergoing a posterior cervical lymph node excision for persistent lymphadenopathy. Examination highlights specific muscle involvement and EMG shows selective denervation. What clinical features and electrodiagnostic findings should guide your approach to this acute postoperative neurologic deficit? How do you localize nerve injuries after neck procedures? VIDEO INFO Category: Peripheral Neuroanatomy, Human Anatomy, USMLE Step 1 Difficulty: Expert - Expert level - For those seeking deep understanding Question Type: Treatment - Evaluate therapeutic interventions and management Case Type: Tricky Findings Explore more ways to learn on this and other topics by going to https://endlessmedical.academy/auth?h... QUESTION A 48-year-old woman presents 48 hours after an open excisional biopsy of a right posterior cervical lymph node performed for persistent, painless lymphadenopathy that had been nondiagnostic on an ultrasound-guided core needle biopsy 1 week earlier. She reports new shoulder girdle pain, difficulty abducting the right arm above shoulder level, a sensation that her shoulder is drooping, and worsening scapular asymmetry when she tries to reach forward. She denies dysphonia or dysphagia.... OPTIONS A. Arrange early surgical exploration of the spinal accessory nerve within weeks using intraoperative nerve action potential-guided strategy (neurolysis if in continuity with recordable NAP; end-to-end repair or interposition graft if discontinuity), combined with immediate scapular-stabilization ph... B. Pursue nonoperative management alone for 6-12 months with scapular-stabilization physiotherapy and external bracing, reserving surgical exploration only if no improvement after a full year given possible delayed spontaneous recovery. C. Inject botulinum toxin into the pectoralis minor and rhomboids with scapular taping to rebalance scapulothoracic rhythm, deferring any nerve exploration because accessory neuropathies typically recover without intervention. D. Schedule arthroscopic subacromial decompression with acromioplasty and corticosteroid injections for presumed rotator cuff impingement, while avoiding exploration of the posterior cervical triangle to reduce iatrogenic risk. CORRECT ANSWER A. Arrange early surgical exploration of the spinal accessory nerve within weeks using intraoperative nerve action potential-guided strategy (neurolysis if in continuity with recordable NAP; end-to-end repair or interposition graft if discontinuity), combined with immediate scapular-stabilization physical therapy; perform as outpatient day surgery under general anesthesia with postoperative PT protocol. EXPLANATION Arrange early surgical exploration of the spinal accessory nerve within weeks using intraoperative nerve action potential-guided strategy (neurolysis if in continuity with recordable NAP; end-to-end repair or interposition graft if discontinuity), combined with immediate scapular-stabilization physical therapy; perform as outpatient day surgery under general anesthesia with postoperative PT protocol. This is correct because the presentation localizes to an iatrogenic spinal accessory nerve (SAN, CN XI) lesion in the posterior cervical triangle after open nodal excision, with classic findings of trapezius weakness, shoulder droop, and scapular dyskinesis while preserving deltoid and rotator cuff innervation.... Further reading: Links to sources are provided for optional further reading only. The questions and explanations are independently authored and do not reproduce or adapt any specific third-party text or content. --------------------------------------------------- Our cases and questions come from the https://EndlessMedical.Academy quiz engine - multi-model platform. Each question and explanation is forged by consensus between multiple top AI models (i.e. Open AI GPT, Claude, Grok, etc.), with automated web searches for the latest research and verified references. Calculations (e.g. eGFR, dosages) are checked via code execution to eliminate errors, and all references are reviewed by several AIs to minimize hallucinations. Important note: This material is entirely AI-generated and has not been verified by human experts; despite stringent consensus checks, perfect accuracy cannot be guaranteed. Exercise caution - always corroborate the content with trusted references or qualified professionals, and never apply information from this content to patient care or clinical decisions without independent verification. Clinicians already rely on AI and online tools - myself included - so treat this content as an additional focused aid, not a replacement for proper medical education. Visit https://endlessmedical.academy for more AI-supported resources and cases. This material can not be treated as medical advice. May contain errors. ------------------...
Comments