Case 189: Manual of CTO PCI - Three (complications) in one (patient) скачать в хорошем качестве
Case 189: Manual of CTO PCI - Three (complications) in one (patient)
3 года назад
Не удается загрузить Youtube-плеер. Проверьте блокировку Youtube в вашей сети.
Повторяем попытку...
Повторяем попытку...
Скачать видео с ютуб по ссылке или смотреть без блокировок на сайте: Case 189: Manual of CTO PCI - Three (complications) in one (patient) в качестве 4k
У нас вы можете посмотреть бесплатно Case 189: Manual of CTO PCI - Three (complications) in one (patient) или скачать в максимальном доступном качестве, видео которое было загружено на ютуб. Для загрузки выберите вариант из формы ниже:
-
Информация по загрузке:
Скачать mp3 с ютуба отдельным файлом. Бесплатный рингтон Case 189: Manual of CTO PCI - Three (complications) in one (patient) в формате MP3:
Если кнопки скачивания не
загрузились
НАЖМИТЕ ЗДЕСЬ или обновите страницу
Если возникают проблемы со скачиванием видео, пожалуйста напишите в поддержку по адресу внизу
страницы.
Спасибо за использование сервиса ClipSaver.ru
Case 189: Manual of CTO PCI - Three (complications) in one (patient)
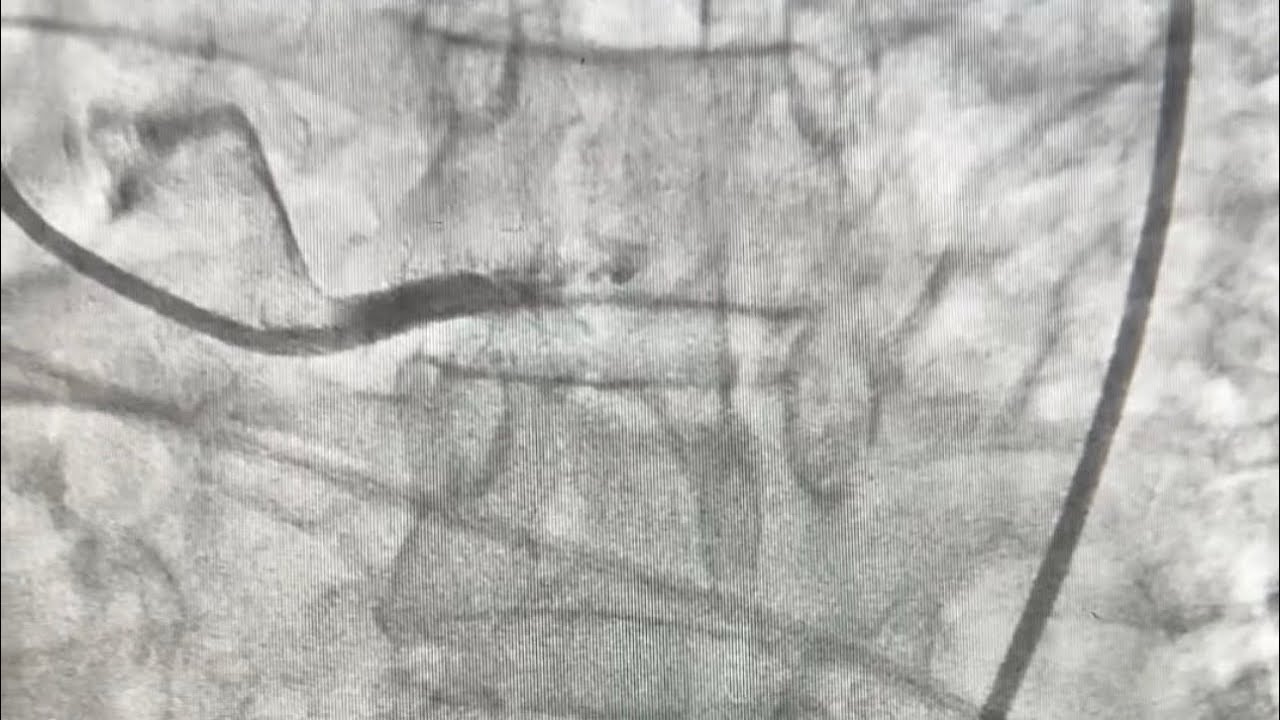
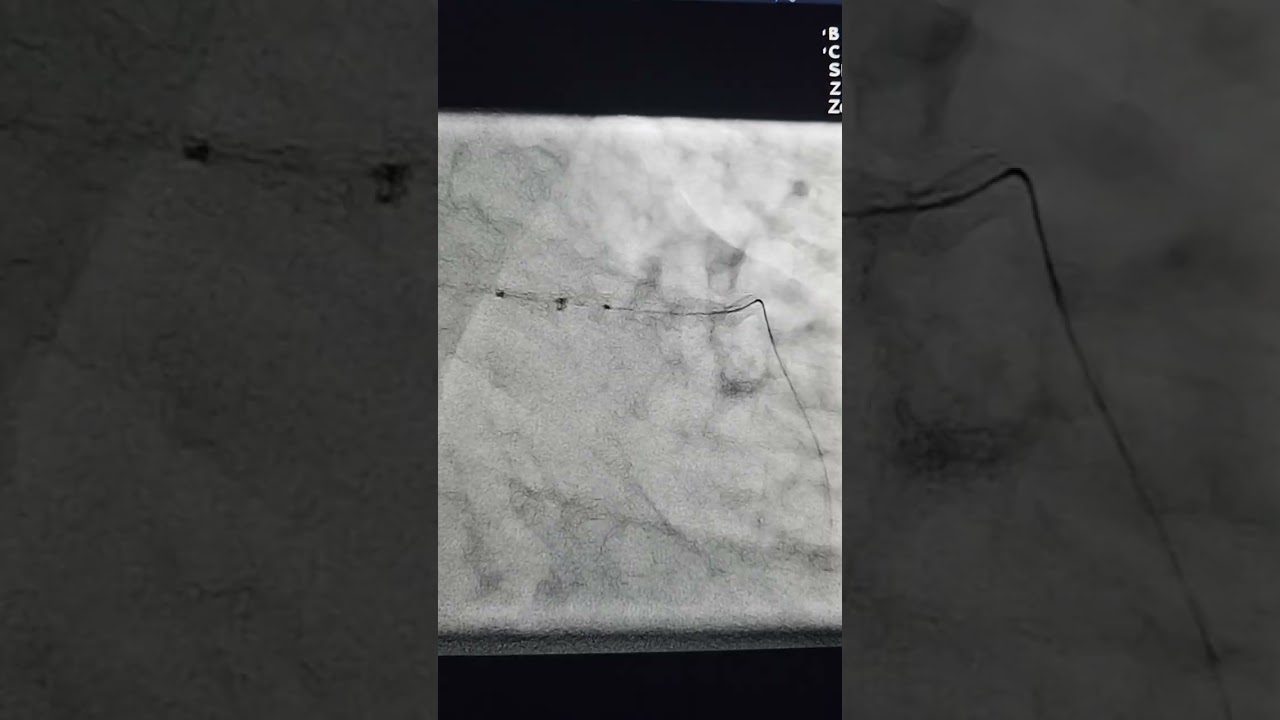
A prior CABG patient was referred for PCI of a right coronary artery in-stent CTO for medically refractory angina. He had occlusion of a sequential SVG to the PDA-posterolateral. Triple injection showed a well defined but blunt proximal cap, long occlusion length into the mid PDA and the right posterolateral. Attempts to cross the proximal cap with a Pilot 200, Gaia Next 2 and Hornet 14 wire failed. The Carlino technique was performed followed by successful advancement of a knuckle past the proximal cap outside the prior stent. The knuckle was advanced to the right posterolateral but delivery of two Stingray balloons failed despite predilation of the RCA and use of an 8 French Trapliner. A ReCross microcatheter was advanced to the right posterolateral but it then became apparent that the catheter had exited from the vessel. The wire was withdrawn and redirected into the posterolateral but we had again difficulty delivering a Stingray balloon and in the process wire position was lost. We switched the original guide catheter (100 cm long 8 French AL1) to a 90 cm long 8 French AL1 guide catheter. After predilation we advanced a new Stingray balloon to the right posterolateral and re-entered into the distal true lumen using the double-blind stick and swap technique. After predilation we saw a perforation of the right posterolateral. We attempted to deliver a 2.5x15 mm PK Papyrus that came off the balloon but was fortunately retrieved. Despite repeated balloon dilations we were unable to deliver two PK Papyrus stents. We used the ping pong technique and eventually were able to deliver a 7 French Guideliner to the right posterolateral through which a PK Papyrus stent was successfully delivered, sealing the perforation. After stenting another perforation was seen in the distal RCA that required implantation of a 3.5 mm PK Papyrus covered stent. The patient became hypotensive with ST segment depression due to slow flow through the SVG skip graft (likely dissection). The SVG was rewired and a 2.5x15 mm DES was delivered through a 6 French Telescope restoring TIMI 3 antegrade flow. Another PK Papyrus stent was delivered to the distal RCA with a nice final result.
Comments