Upper Limb Anatomy, Human Anatomy, USMLE Step 1 - Full Vignette with Extended Explanations скачать в хорошем качестве
Upper Limb Anatomy, Human Anatomy, USMLE Step 1 - Full Vignette with Extended Explanations
12 дней назад
Не удается загрузить Youtube-плеер. Проверьте блокировку Youtube в вашей сети.
Повторяем попытку...
Повторяем попытку...
Скачать видео с ютуб по ссылке или смотреть без блокировок на сайте: Upper Limb Anatomy, Human Anatomy, USMLE Step 1 - Full Vignette with Extended Explanations в качестве 4k
У нас вы можете посмотреть бесплатно Upper Limb Anatomy, Human Anatomy, USMLE Step 1 - Full Vignette with Extended Explanations или скачать в максимальном доступном качестве, видео которое было загружено на ютуб. Для загрузки выберите вариант из формы ниже:
-
Информация по загрузке:
Скачать mp3 с ютуба отдельным файлом. Бесплатный рингтон Upper Limb Anatomy, Human Anatomy, USMLE Step 1 - Full Vignette with Extended Explanations в формате MP3:
Если кнопки скачивания не
загрузились
НАЖМИТЕ ЗДЕСЬ или обновите страницу
Если возникают проблемы со скачиванием видео, пожалуйста напишите в поддержку по адресу внизу
страницы.
Спасибо за использование сервиса ClipSaver.ru
Upper Limb Anatomy, Human Anatomy, USMLE Step 1 - Full Vignette with Extended Explanations
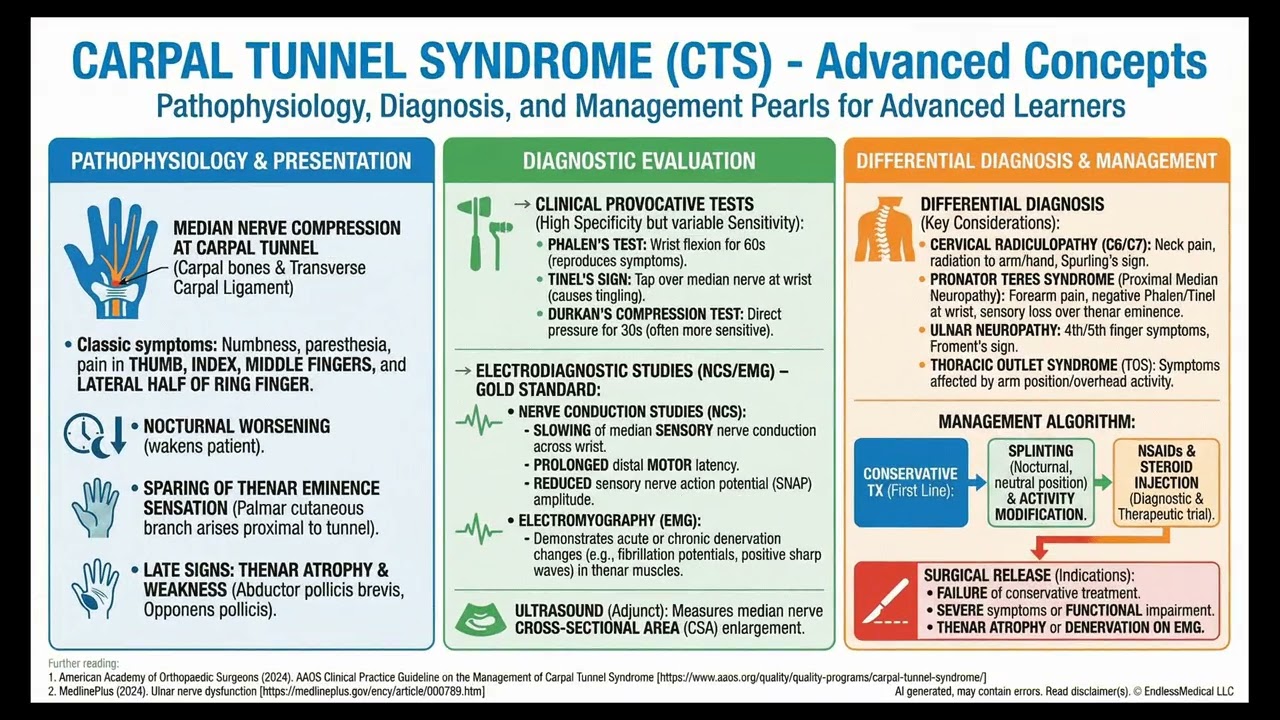
Several patients arrive at a family clinic with complaints of hand pain and numbness, each displaying unique patterns of symptoms, physical exam findings, and daily activity risks. How can clinical presentation and specific neurological signs help distinguish the underlying condition? What physical exam maneuvers and sensory findings are essential to accurately identify the source of their symptoms? VIDEO INFO Category: Upper Limb Anatomy, Human Anatomy, USMLE Step 1 Difficulty: Easy - Basic level - Suitable for medical students Question Type: Differential Physical History Case Type: Multi Patient Explore more ways to learn on this and other topics by going to https://endlessmedical.academy/auth?h... QUESTION "Four patients come to a family clinic on the same day for numbness and hand pain. Vitals are checked first. All have temperature 36.1 degreesC, oxygen saturation 100%, and normal blood pressure near 117/62 mm Hg.... OPTIONS A. Patient A, with night paresthesia in the thumb, index, and middle fingers plus positive wrist Tinel and Phalen tests and mild thenar weakness, consistent with median nerve compression. B. Patient B, with ulnar-sided paresthesia, interossei weakness, and positive Froment sign localizing to cubital tunnel ulnar neuropathy rather than median nerve compression. C. Patient C, with radial styloid pain and positive Finkelstein maneuver consistent with de Quervain tenosynovitis and not a median neuropathy. D. Patient D, with dorsal web-space sensory loss and wrist drop localizing to radial nerve palsy after compression in the spiral groove, not a median neuropathy. Symptoms began after sleeping on a bench with the arm draped over the chair back. CORRECT ANSWER A. Patient A, with night paresthesia in the thumb, index, and middle fingers plus positive wrist Tinel and Phalen tests and mild thenar weakness, consistent with median nerve compression. EXPLANATION Patient A s nocturnal paresthesia in the thumb, index, and middle fingers, phone-dropping, positive Tinel and Phalen at the wrist, and mild thenar weakness fit median nerve compression in the carpal tunnel. Shaking her hand for relief is typical; two-point discrimination reduction at the index fingertip supports median sensory involvement. These findings match clinical criteria used to diagnose carpal tunnel syndrome without mandatory ancillary testing, reflecting contemporary guidance. Patients B, C, and D each have non-median localizations. Patient B reports ulnar-sided symptoms (little finger and half ring finger), interossei weakness, and Froment sign, all pointing to ulnar neuropathy at the cubital tunnel. Patient C s radial styloid pain, first dorsal compartment tenderness, and positive Finkelstein maneuver are classic for de Quervain tenosynovitis with normal finger sensation. Patient D shows wrist drop with dorsal web-space sensory loss after compression during sleep, characteristic of radial nerve palsy in the spiral groove. These presentations exclude median neuropathy despite some overlapping hand discomfort. In summary, the correct answer is Patient A, whose symptom distribution, provocative tests, and subtle thenar involvement are prototypical for carpal tunnel syndrome. Teaching points: Median neuropathy causes thumb-middle finger paresthesia with nocturnal worsening and positive Phalen/Tinel. Ulnar neuropathy localizes to the cubital tunnel with Froment sign; de Quervain is a tendon sheath disorder; radial palsy causes wrist drop and dorsal web-space sensory loss. Further reading: Links to sources are provided for optional further reading only. The questions and explanations are independently authored and do not reproduce or adapt any specific third-party text or content. --------------------------------------------------- Our cases and questions come from the https://EndlessMedical.Academy quiz engine - multi-model platform. Each question and explanation is forged by consensus between multiple top AI models (i.e. Open AI GPT, Claude, Grok, etc.), with automated web searches for the latest research and verified references. Calculations (e.g. eGFR, dosages) are checked via code execution to eliminate errors, and all references are reviewed by several AIs to minimize hallucinations. Important note: This material is entirely AI-generated and has not been verified by human experts; despite stringent consensus checks, perfect accuracy cannot be guaranteed. Exercise caution - always corroborate the content with trusted references or qualified professionals, and never apply information from this content to patient care or clinical decisions without independent verification. Clinicians already rely on AI and online tools - myself included - so treat this content as an additional focused aid, not a replacement for proper medical education. Visit https://endlessmedical.academy for more AI-supported resources and cases. This material can not be treated as medical advice. May contain errors. -----
Comments



















