Ectasia Treatment CXL, TE PTK, topography guided treatment, intracorneal ring segments - Reinstein скачать в хорошем качестве
Ectasia Treatment CXL, TE PTK, topography guided treatment, intracorneal ring segments - Reinstein
8 месяцев назад
Не удается загрузить Youtube-плеер. Проверьте блокировку Youtube в вашей сети.
Повторяем попытку...
Повторяем попытку...
Скачать видео с ютуб по ссылке или смотреть без блокировок на сайте: Ectasia Treatment CXL, TE PTK, topography guided treatment, intracorneal ring segments - Reinstein в качестве 4k
У нас вы можете посмотреть бесплатно Ectasia Treatment CXL, TE PTK, topography guided treatment, intracorneal ring segments - Reinstein или скачать в максимальном доступном качестве, видео которое было загружено на ютуб. Для загрузки выберите вариант из формы ниже:
-
Информация по загрузке:
Скачать mp3 с ютуба отдельным файлом. Бесплатный рингтон Ectasia Treatment CXL, TE PTK, topography guided treatment, intracorneal ring segments - Reinstein в формате MP3:
Если кнопки скачивания не
загрузились
НАЖМИТЕ ЗДЕСЬ или обновите страницу
Если возникают проблемы со скачиванием видео, пожалуйста напишите в поддержку по адресу внизу
страницы.
Спасибо за использование сервиса ClipSaver.ru
Ectasia Treatment CXL, TE PTK, topography guided treatment, intracorneal ring segments - Reinstein
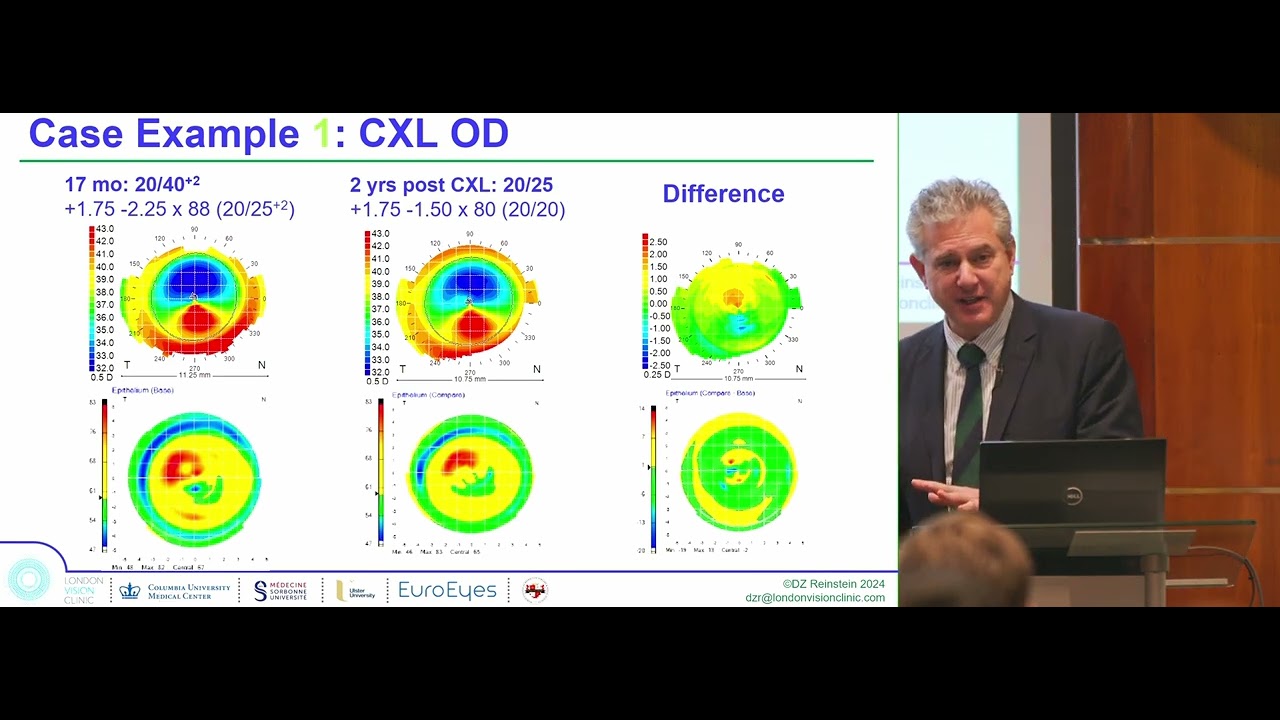
London Vision Clinic Forefront Therapeutic Course 2024 – Keratoconus Lecture Keratoconus is a condition where the cornea—the clear window at the front of the eye—becomes thinner and bulges into a cone-like shape. For patients this means blurred or distorted vision, glare, ghosting and frustration with glasses or contact lenses. For surgeons it remains one of the most complex challenges in corneal and refractive surgery, demanding a balance of biomechanics, optics and patient safety. In this lecture, Professor Dan Reinstein explains how keratoconus can be diagnosed, monitored and treated using epithelial thickness mapping, difference topography maps and modern combinations of corneal cross-linking (CXL), transepithelial phototherapeutic keratectomy (PTK) and topography-guided excimer ablation. The talk is designed to make sense for both patients and colleagues: clear, plain explanations for those seeking answers, and detailed technical insights for surgeons. What keratoconus feels like vs. what it looks like Patients may first notice ghosting, haloes at night or glasses that never feel strong enough. Surgeons see the matching patterns on scans: localised steepening, posterior elevation and characteristic epithelial thinning directly over the cone. Reinstein’s research has shown that epithelial mapping can reveal disease earlier than topography alone. Why follow-up matters Patients sometimes ask: “If I can see well, why do I need scans?” Keratoconus can progress silently. Even with 20/20 vision, difference maps may reveal subtle steepening. Surgeons understand that a quarter dioptre of cylinder can mean real biomechanical change—hence the need for serial tomography. Cross-linking: the foundation For patients, CXL is the only proven treatment to halt keratoconus. Riboflavin drops plus UV light stiffen corneal collagen like adding steel to concrete, often preventing the need for corneal transplant. Surgeons know the nuances: Dresden protocol versus accelerated protocols, Reinstein’s 7–8 minute compromise with the Avedro system, and the danger of combining mitomycin C with CXL, which can trigger deep haze. Long-term monitoring remains essential as refraction can shift hyperopically over time. Beyond stabilisation – improving vision Some patients gain clearer sight after CXL, but its main role is stabilisation. Surgeons can enhance outcomes with combinations: – PTK + CXL to unmask and reduce cone height. – Topography-guided ablation + CXL (Athens Protocol) to regularise the cornea then lock it in. – PTK + Topography-guided + CXL for maximal cone reduction. Eye rubbing For patients: rubbing your eyes can make keratoconus worse. The cornea behaves like a balloon—rub it and it stretches. Surgeons know this is not anecdotal: high IOP, deep resection and eye rubbing were identified decades ago as risk factors for ectasia. Case examples Real patients illustrate both risk and hope: a young high myope developing ectasia after SMILE, stabilised with CXL; a 26-year-old with subtle astigmatic progression improved after CXL; post-LASIK ectasia managed safely using “free tissue” in the flap. Centration principles Patients may not ask, but surgeons know: treatments should never be centred on the pupil, which shifts with light. The stable reference is the corneal vertex. Future directions Questions remain: what is the safest ablation depth, how durable are accelerated CXL protocols over decades, can intracorneal ring nomograms be standardised? Patients should understand keratoconus requires lifelong follow-up. Surgeons recognise that protocols continue to evolve. Conclusion For patients: keratoconus is treatable. Cross-linking can stop progression and combined techniques can improve vision. Avoid eye rubbing and attend long-term follow-up. For surgeons: difference maps and epithelial mapping are essential, consistent CXL protocols matter, and combination strategies offer the most powerful results. Keywords: keratoconus, keratoconus treatment, keratoconus surgery, corneal cross-linking, CXL, transepithelial PTK, phototherapeutic keratectomy, topography-guided ablation, Athens protocol, ectasia after LASIK, ectasia after SMILE, keratoconus eye rubbing, corneal epithelial mapping, difference maps, keratoconus explained, keratoconus vision correction, corneal transplant alternatives.
Comments