Module 25.3 - Caustic Ingestions - Lecture скачать в хорошем качестве
Module 25.3 - Caustic Ingestions - Lecture
2 часа назад
Не удается загрузить Youtube-плеер. Проверьте блокировку Youtube в вашей сети.
Повторяем попытку...
Повторяем попытку...
Скачать видео с ютуб по ссылке или смотреть без блокировок на сайте: Module 25.3 - Caustic Ingestions - Lecture в качестве 4k
У нас вы можете посмотреть бесплатно Module 25.3 - Caustic Ingestions - Lecture или скачать в максимальном доступном качестве, видео которое было загружено на ютуб. Для загрузки выберите вариант из формы ниже:
-
Информация по загрузке:
Скачать mp3 с ютуба отдельным файлом. Бесплатный рингтон Module 25.3 - Caustic Ingestions - Lecture в формате MP3:
Если кнопки скачивания не
загрузились
НАЖМИТЕ ЗДЕСЬ или обновите страницу
Если возникают проблемы со скачиванием видео, пожалуйста напишите в поддержку по адресу внизу
страницы.
Спасибо за использование сервиса ClipSaver.ru
Module 25.3 - Caustic Ingestions - Lecture
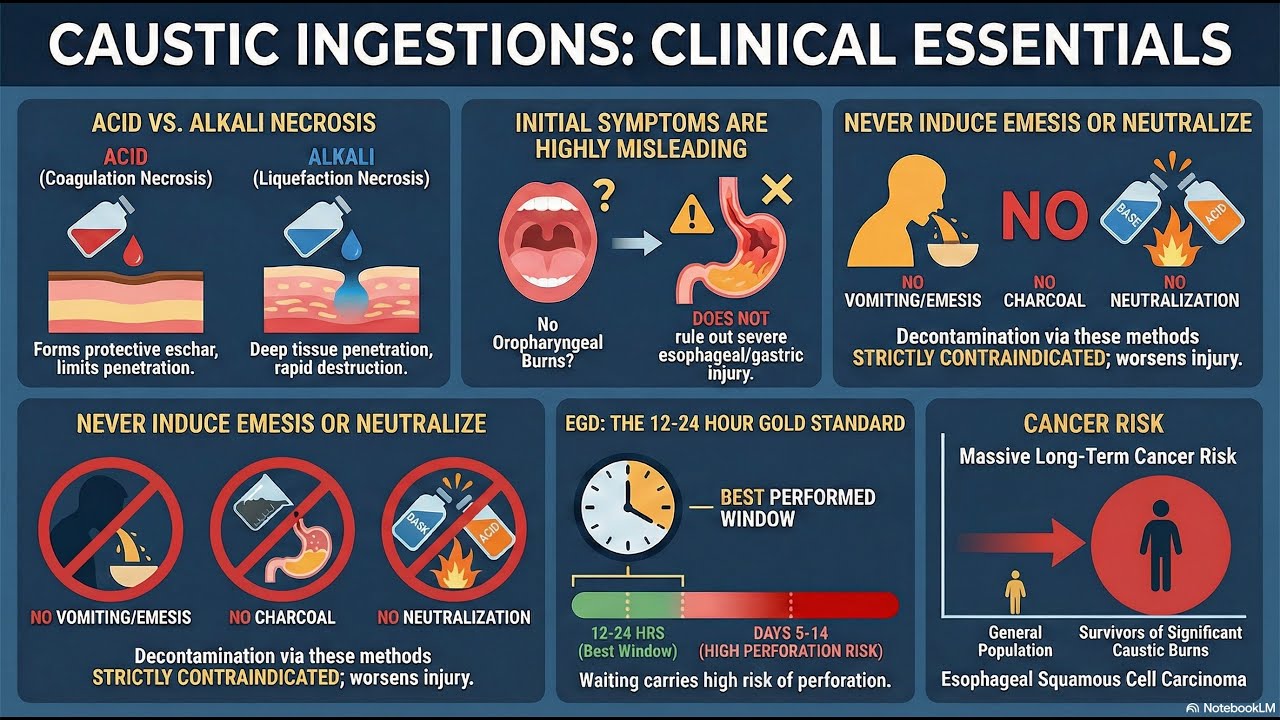
Welcome to Nexus Clinical! Before diving into this lecture, I want to ensure we're all on the same page. This is for general informational purposes only and does not constitute the practice of medicine, nursing, or other professional healthcare services, including the giving of medical advice. No doctor-patient or pharmacist-patient relationship is formed. Using this information and the materials linked to this content is at the user's risk. This is not intended to substitute for professional medical advice, diagnosis, or treatment. Users should not disregard or delay seeking medical advice for any medical condition they have, and they should consult their healthcare professionals for any such conditions. Clinical experts created the references, content, and clinical insight. NotebookLM, a Google AI tool, created the content, which I extensively reviewed before release. Finally, the host states that he takes all conflicts of interest seriously. Currently, there are no conflicts to disclose. For all of his disclosures and the companies he invests in or advises, he directs users to reach out independently, where he keeps an up-to-date and active list of all disclosures. Welcome to this vital toxicology curriculum focusing on Caustic Ingestions. This module provides a comprehensive overview of corrosive exposures, which carry the risk of severe, life-threatening injury and debilitating long-term complications. Key Learning Objectives: Pathophysiology: Understand the difference between alkaline injury (liquefaction necrosis, permitting deeper penetration) and acidic injury (coagulation necrosis, forming an eschar). Injury severity is critically influenced by pH, concentration, and the physical state of the agent. Clinical Assessment: Clinicians must remember that initial symptoms are highly unreliable predictors of internal injury severity. Signs of airway compromise, such as stridor or hoarseness, constitute an immediate emergency. Diagnosis: Esophagogastroduodenoscopy (EGD) is the diagnostic gold standard, ideally performed within 12–24 hours post-ingestion to grade the injury using the Zargar classification. Contrast-enhanced CT serves as a crucial adjunct for detecting perforation or assessing transmural damage. Acute Management: Immediate priority is airway protection and hemodynamic stabilization. Induced emesis, activated charcoal (except for specific cationic metal toxins like ZnCl2/HgCl2), and neutralization are generally contraindicated. Corticosteroids remain highly debated, but evidence suggests a potential role in reducing stricture risk for patients with Grade IIb circumferential esophageal burns. Emergency surgery is required for perforation or extensive necrosis (Grade III). Long-Term Follow-up: Long-term management involves treating strictures (primarily via endoscopic dilation) and maintaining lifelong surveillance for esophageal squamous cell carcinoma, a risk that is substantially increased (up to 1000-fold) following severe caustic injury. Effective management requires a comprehensive, multidisciplinary team approach for optimal patient outcomes.
Comments
-
 8 минут назад
8 минут назад
-
 1 день назад
1 день назад
-
 Трансляция закончилась 3 дня назад
Трансляция закончилась 3 дня назад
-
 3 дня назад
3 дня назад
-
 4 дня назад
4 дня назад
-
 1 месяц назад
1 месяц назад
-
 2 месяца назад
2 месяца назад
-
 1 месяц назад
1 месяц назад
-
 2 дня назад
2 дня назад
-
 Трансляция закончилась 2 недели назад
Трансляция закончилась 2 недели назад
-
 1 час назад
1 час назад
-
 6 часов назад
6 часов назад
-
 4 дня назад
4 дня назад
-
 1 месяц назад
1 месяц назад
-
 8 дней назад
8 дней назад
-
 3 дня назад
3 дня назад
-
 2 недели назад
2 недели назад
-
 5 дней назад
5 дней назад
-
 2 недели назад
2 недели назад
-
 1 месяц назад
1 месяц назад