Prognostic Factors Evaluation, Immunoglobulin A (IgA) Nephropathy, Glomerulonephritis: Causes, Diagn скачать в хорошем качестве
Prognostic Factors Evaluation, Immunoglobulin A (IgA) Nephropathy, Glomerulonephritis: Causes, Diagn
21 час назад
Не удается загрузить Youtube-плеер. Проверьте блокировку Youtube в вашей сети.
Повторяем попытку...
Повторяем попытку...
Скачать видео с ютуб по ссылке или смотреть без блокировок на сайте: Prognostic Factors Evaluation, Immunoglobulin A (IgA) Nephropathy, Glomerulonephritis: Causes, Diagn в качестве 4k
У нас вы можете посмотреть бесплатно Prognostic Factors Evaluation, Immunoglobulin A (IgA) Nephropathy, Glomerulonephritis: Causes, Diagn или скачать в максимальном доступном качестве, видео которое было загружено на ютуб. Для загрузки выберите вариант из формы ниже:
-
Информация по загрузке:
Скачать mp3 с ютуба отдельным файлом. Бесплатный рингтон Prognostic Factors Evaluation, Immunoglobulin A (IgA) Nephropathy, Glomerulonephritis: Causes, Diagn в формате MP3:
Если кнопки скачивания не
загрузились
НАЖМИТЕ ЗДЕСЬ или обновите страницу
Если возникают проблемы со скачиванием видео, пожалуйста напишите в поддержку по адресу внизу
страницы.
Спасибо за использование сервиса ClipSaver.ru
Prognostic Factors Evaluation, Immunoglobulin A (IgA) Nephropathy, Glomerulonephritis: Causes, Diagn
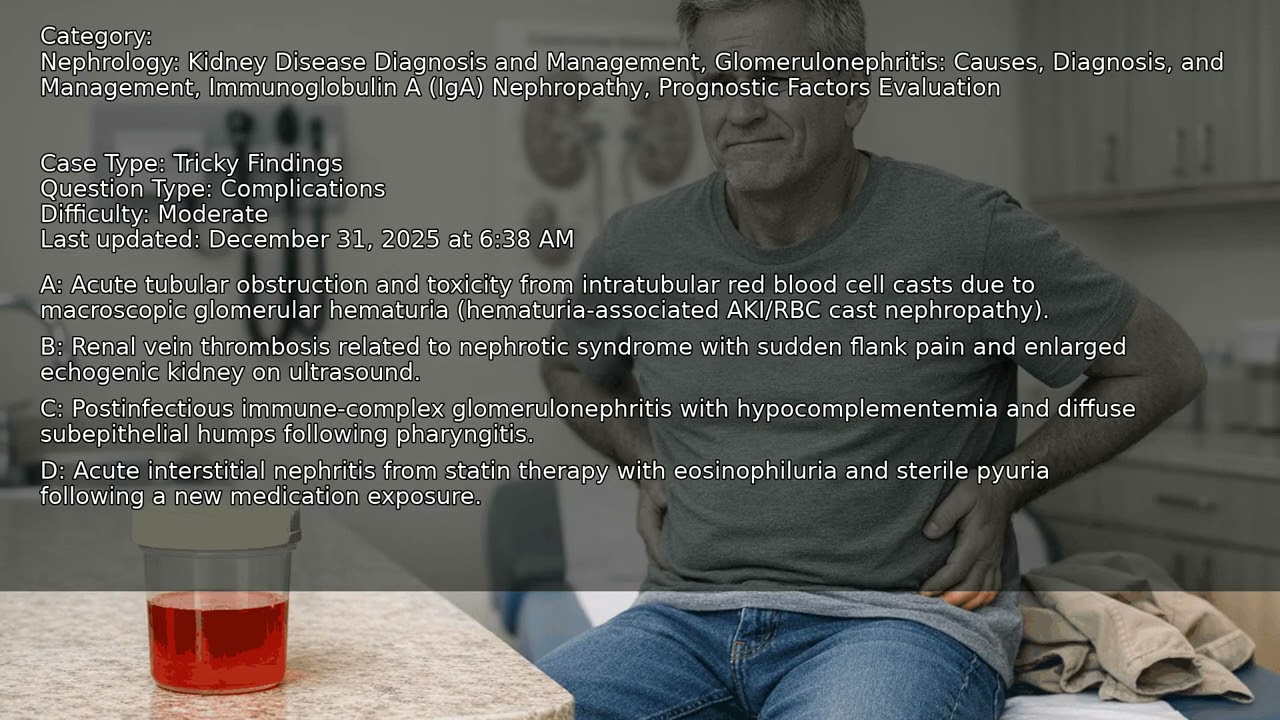
A 56-year-old man with a history of primary IgA nephropathy presents with severe bilateral flank pain and persistent gross hematuria following an upper-respiratory infection. Despite hydration and stable vital signs, his kidney function worsens, and urinalysis reveals dysmorphic RBCs with prominent casts. What clinical reasoning steps are crucial in evaluating new-onset kidney dysfunction in a patient with chronic glomerular disease who develops acute symptoms after an infection? VIDEO INFO Category: Prognostic Factors Evaluation, Immunoglobulin A (IgA) Nephropathy, Glomerulonephritis: Causes, Diagnosis, and Management, Nephrology: Kidney Disease Diagnosis and Management Difficulty: Moderate - Intermediate level - Requires solid foundational knowledge Question Type: Complications Case Type: Tricky Findings Explore more ways to learn on this and other topics by going to https://endlessmedical.academy/auth?h... QUESTION A 56-year-old man with biopsy-proven primary IgA nephropathy (diagnosed 18 months ago) presents with 48 hours of gross hematuria and severe bilateral flank pain after an upper-respiratory infection.... OPTIONS A. Acute tubular obstruction and toxicity from intratubular red blood cell casts due to macroscopic glomerular hematuria (hematuria-associated AKI/RBC cast nephropathy). B. Postinfectious immune-complex glomerulonephritis with hypocomplementemia and diffuse subepithelial humps following pharyngitis. C. Renal vein thrombosis related to nephrotic syndrome with sudden flank pain and enlarged echogenic kidney on ultrasound. D. Acute interstitial nephritis from statin therapy with eosinophiluria and sterile pyuria following a new medication exposure. CORRECT ANSWER A. Acute tubular obstruction and toxicity from intratubular red blood cell casts due to macroscopic glomerular hematuria (hematuria-associated AKI/RBC cast nephropathy). EXPLANATION "Acute tubular obstruction and toxicity from intratubular red blood cell casts due to macroscopic glomerular hematuria (hematuria-associated AKI/RBC cast nephropathy)." - In IgA nephropathy, gross hematuria can precipitate acute kidney injury when red blood cells flood the tubules, aggregate with Tamm-Horsfall protein, and form obstructive casts; heme and iron catalyze oxidative tubular injury. This patient s timing (post-upper respiratory infection), persistent gross hematuria, rising creatinine, abundant RBC casts, and normal complements with negative streptococcal studies fit hematuria-associated AKI and argue against postinfectious GN. Ultrasound without hydronephrosis makes obstructive uropathy unlikely; lack of nephrotic syndrome and a normal ultrasound argue against renal vein thrombosis; absence of eosinophiluria or new drug exposure argues against acute interstitial nephritis. In summary, hematuria-associated tubular obstruction/toxicity from RBC casts best explains the abrupt creatinine rise during ongoing gross hematuria in IgA nephropathy. Key teaching points: macroscopic hematuria can cause AKI via RBC cast obstruction and heme toxicity; complements are typically normal in IgA nephropathy; management centers on supportive care, hemodynamic optimization, analgesia that avoids NSAIDs, and timely escalation to dialysis if indicated. Further reading: Links to sources are provided for optional further reading only. The questions and explanations are independently authored and do not reproduce or adapt any specific third-party text or content. --------------------------------------------------- Our cases and questions come from the https://EndlessMedical.Academy quiz engine - multi-model platform. Each question and explanation is forged by consensus between multiple top AI models (i.e. Open AI GPT, Claude, Grok, etc.), with automated web searches for the latest research and verified references. Calculations (e.g. eGFR, dosages) are checked via code execution to eliminate errors, and all references are reviewed by several AIs to minimize hallucinations. Important note: This material is entirely AI-generated and has not been verified by human experts; despite stringent consensus checks, perfect accuracy cannot be guaranteed. Exercise caution - always corroborate the content with trusted references or qualified professionals, and never apply information from this content to patient care or clinical decisions without independent verification. Clinicians already rely on AI and online tools - myself included - so treat this content as an additional focused aid, not a replacement for proper medical education. Visit https://endlessmedical.academy for more AI-supported resources and cases. This material can not be treated as medical advice. May contain errors. ---------------------------------------------------
Comments
-
 4 года назад
4 года назад
-
 3 года назад
3 года назад
-
 Трансляция закончилась 7 месяцев назад
Трансляция закончилась 7 месяцев назад
-
 2 часа назад
2 часа назад
-
 10 часов назад
10 часов назад
-
 2 года назад
2 года назад
-
 4 часа назад
4 часа назад
-
 2 года назад
2 года назад
-
 9 минут назад
9 минут назад
-
 3 недели назад
3 недели назад
-
 Трансляция закончилась 1 год назад
Трансляция закончилась 1 год назад
-
 Трансляция закончилась 1 месяц назад
Трансляция закончилась 1 месяц назад
-
 2 года назад
2 года назад
-
 5 лет назад
5 лет назад
-
 3 недели назад
3 недели назад
-
 4 года назад
4 года назад
-
 1 месяц назад
1 месяц назад
-
 16 часов назад
16 часов назад
-
 3 часа назад
3 часа назад
-
 3 месяца назад
3 месяца назад