Ocular Manifestation in Obstructive sleep apnea, what is the role of a good ophthalmologist скачать в хорошем качестве
Ocular Manifestation in Obstructive sleep apnea, what is the role of a good ophthalmologist
2 месяца назад
Не удается загрузить Youtube-плеер. Проверьте блокировку Youtube в вашей сети.
Повторяем попытку...
Повторяем попытку...

Скачать видео с ютуб по ссылке или смотреть без блокировок на сайте: Ocular Manifestation in Obstructive sleep apnea, what is the role of a good ophthalmologist в качестве 4k
У нас вы можете посмотреть бесплатно Ocular Manifestation in Obstructive sleep apnea, what is the role of a good ophthalmologist или скачать в максимальном доступном качестве, видео которое было загружено на ютуб. Для загрузки выберите вариант из формы ниже:
-
Информация по загрузке:
Скачать mp3 с ютуба отдельным файлом. Бесплатный рингтон Ocular Manifestation in Obstructive sleep apnea, what is the role of a good ophthalmologist в формате MP3:
Если кнопки скачивания не
загрузились
НАЖМИТЕ ЗДЕСЬ или обновите страницу
Если возникают проблемы со скачиванием видео, пожалуйста напишите в поддержку по адресу внизу
страницы.
Спасибо за использование сервиса ClipSaver.ru
Ocular Manifestation in Obstructive sleep apnea, what is the role of a good ophthalmologist
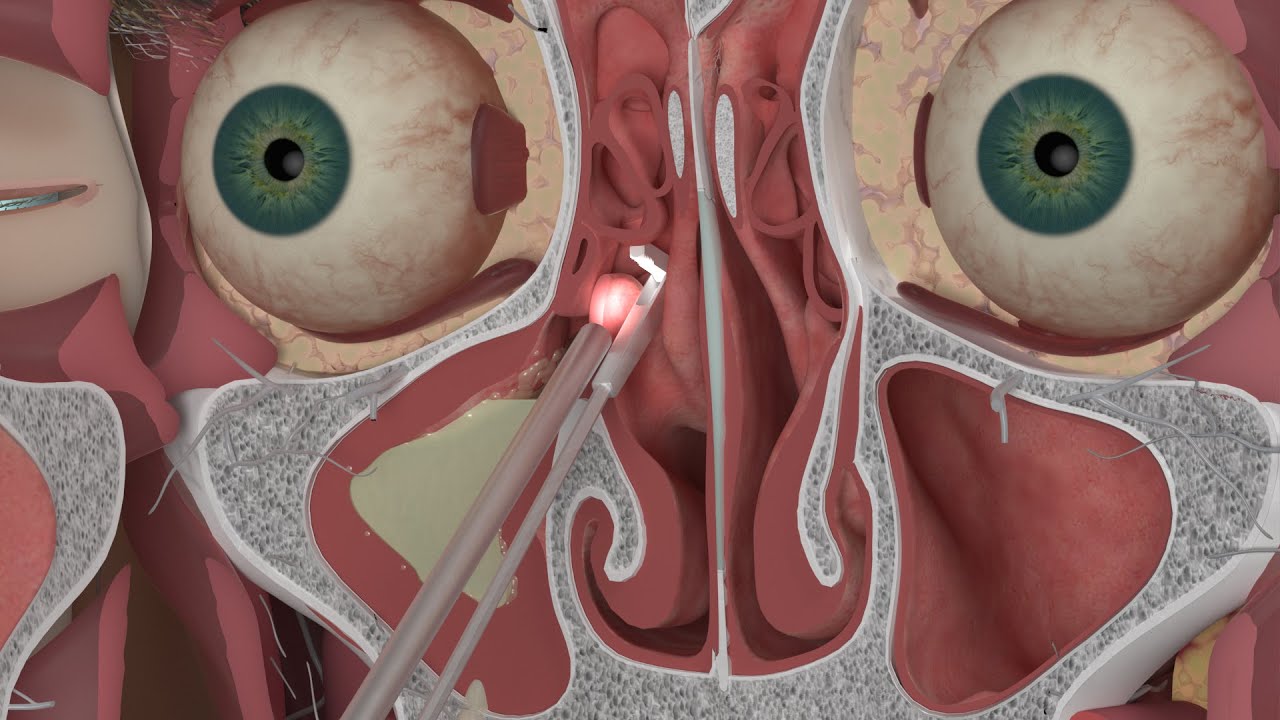
Obstructive sleep apnea is a highly prevalent but widely underdiagnosed disorder characterized by repeated episodes of upper airway collapse during sleep. These episodes result in intermittent hypoxia, hypercapnia, and significant sleep fragmentation. Globally, it is estimated that more than one billion individuals suffer from some degree of sleep-disordered breathing, with prevalence especially high among men, individuals with obesity, and those with craniofacial or neuromuscular disorders. In many regions, despite regular interaction with healthcare providers, the majority of Obstructive sleep apnea cases remain undetected, making awareness and multidisciplinary screening essential. The diagnosis of Obstructive sleep apnea relies primarily on polysomnography—an overnight sleep study in which apneas (complete cessation of airflow for ≥10 seconds) and hypopneas (≥30% airflow reduction for ≥10 seconds with desaturation or arousal) are quantified using the Apnea–Hypopnea Index (AHI). Patients with mild disease have an AHI between 5 and 15, moderate disease between 15 and 30, and severe disease above 30 events per hour. For selected adults with a high clinical suspicion, home sleep apnea testing can serve as an effective alternative. New technologies, including peripheral arterial tonometry, AI-assisted oximetry, and acoustic airflow analysis, are improving accessibility and accuracy of sleep assessments. The systemic pathophysiology of Obstructive sleep apnea is multifaceted. Intermittent hypoxia activates oxidative stress pathways and triggers widespread inflammation through cytokines such as IL-6 and TNF-α. Simultaneously, the autonomic nervous system becomes hyperactivated, causing repeated surges in sympathetic tone. These surges release large amounts of catecholamines, producing cycles of nocturnal hypertension followed by rebound hypotension. Over time, this pattern contributes to endothelial dysfunction, impaired nitric-oxide signaling, and vascular stiffness. Metabolic consequences include insulin resistance, dyslipidemia, and increased visceral fat—all of which amplify cardiometabolic disease. These systemic mechanisms also give rise to a self-perpetuating cycle: hypoxia activates sympathetic pathways, sympathetic activation elevates blood pressure, and sustained hypertension damages vascular autoregulation, making tissues—including ocular structures—more vulnerable to ischemia. The ocular manifestations of sleep apnea reflect these underlying processes. One of the most frequent associations is ocular surface disease. Patients with moderate or severe Obstructive sleep apnea commonly exhibit reduced Schirmer scores, increased tear osmolarity, and meibomian gland dysfunction. Contributing factors include mouth breathing, nocturnal lagophthalmos, and low-grade systemic inflammation. Interestingly, continuous positive airway pressure (CPAP) therapy can either improve or worsen symptoms depending on mask fit. When mask leak is controlled, CPAP improves lacrimal gland function and increases tear stability after several months of therapy. Obstructive sleep apnea also has a significant relationship with glaucomatous neurodegeneration. Epidemiologic studies consistently show that patients with Obstructive sleep apnea—especially severe untreated disease—have a higher risk of developing normal-tension glaucoma. Optical coherence tomography (OCT) and OCT-angiography have demonstrated thinning of the retinal nerve fiber layer (RNFL), reduction of ganglion cell layer (GCL) thickness, and decreased macular vessel density in untreated Obstructive sleep apnea patients. These changes correlate strongly with the severity of nocturnal hypoxia. Importantly, several longitudinal studies indicate that effective CPAP therapy leads to stabilization, and in some cases partial improvement, of GCL thickness and peripapillary perfusion, suggesting a neuroprotective benefit. Obstructive sleep apnea is also recognized as a powerful risk factor for non-arteritic anterior ischemic optic neuropathy (NAION). The combination of nocturnal hypotension, impaired optic nerve autoregulation, and oxygen desaturation increases the likelihood of ischemic events, particularly in individuals with “disc at risk” anatomy. Patients with untreated Obstructive sleep apnea are more likely to experience bilateral or sequential NAION, whereas CPAP use has been associated with reduced incidence of fellow-eye involvement. Retinal vascular disorders—including central retinal vein occlusion (CRVO) and central retinal artery occlusion (CRAO)—also occur more frequently in OSA due to venous hypertension, endothelial dysfunction, platelet activation, and embolic tendencies.
Comments