Musculoskeletal, Skin & Subcutaneous Tissue, Physiology, USMLE Step 1 - Full Vignette with Extended скачать в хорошем качестве
Musculoskeletal, Skin & Subcutaneous Tissue, Physiology, USMLE Step 1 - Full Vignette with Extended
15 часов назад
Не удается загрузить Youtube-плеер. Проверьте блокировку Youtube в вашей сети.
Повторяем попытку...
Повторяем попытку...
Скачать видео с ютуб по ссылке или смотреть без блокировок на сайте: Musculoskeletal, Skin & Subcutaneous Tissue, Physiology, USMLE Step 1 - Full Vignette with Extended в качестве 4k
У нас вы можете посмотреть бесплатно Musculoskeletal, Skin & Subcutaneous Tissue, Physiology, USMLE Step 1 - Full Vignette with Extended или скачать в максимальном доступном качестве, видео которое было загружено на ютуб. Для загрузки выберите вариант из формы ниже:
-
Информация по загрузке:
Скачать mp3 с ютуба отдельным файлом. Бесплатный рингтон Musculoskeletal, Skin & Subcutaneous Tissue, Physiology, USMLE Step 1 - Full Vignette with Extended в формате MP3:
Если кнопки скачивания не
загрузились
НАЖМИТЕ ЗДЕСЬ или обновите страницу
Если возникают проблемы со скачиванием видео, пожалуйста напишите в поддержку по адресу внизу
страницы.
Спасибо за использование сервиса ClipSaver.ru
Musculoskeletal, Skin & Subcutaneous Tissue, Physiology, USMLE Step 1 - Full Vignette with Extended
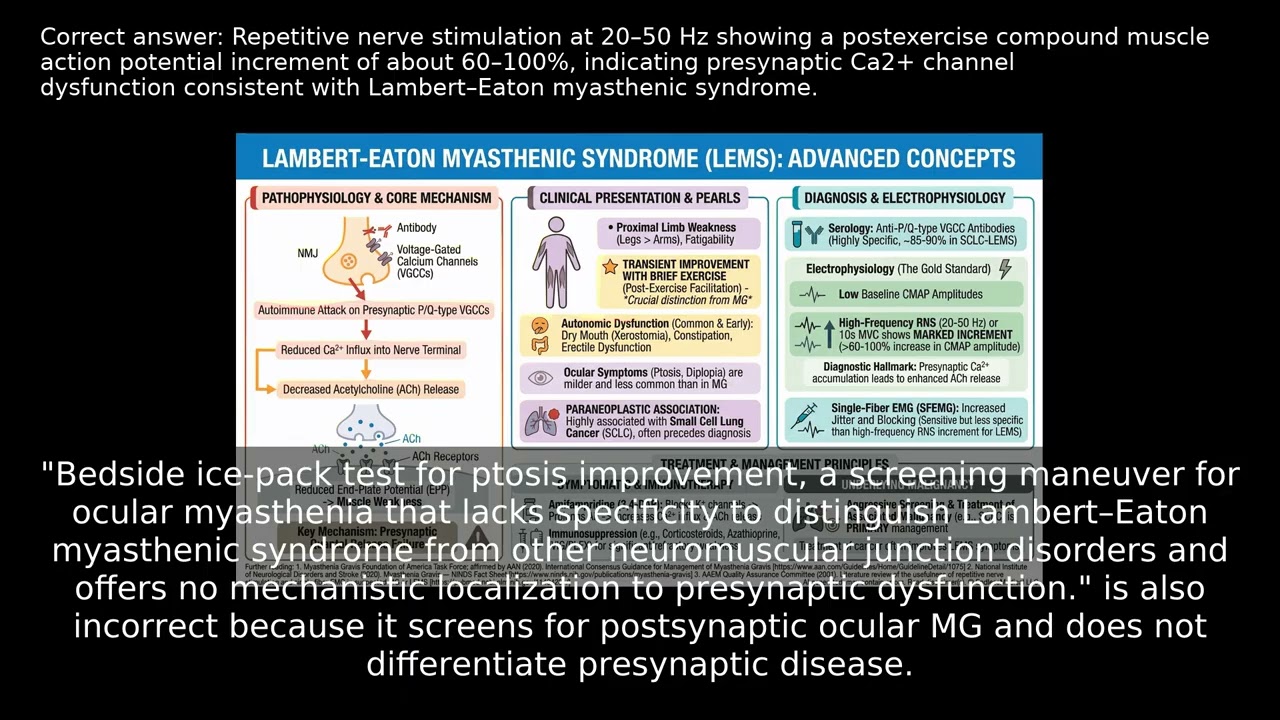
A 27-year-old man reports several months of fluctuating proximal muscle weakness, early fatigability during daily activities, dry mouth, and transient improvement in strength after brief exertion. Neurologic exam shows areflexia with partial resolution after contraction and mild ocular involvement. With this constellation of symptoms, what clinical features and findings help distinguish between different types of neuromuscular junction disorders? How do these presentations guide your diagnostic approach? VIDEO INFO Category: Musculoskeletal, Skin & Subcutaneous Tissue, Physiology, USMLE Step 1 Difficulty: Moderate - Intermediate level - Requires solid foundational knowledge Question Type: Differential Testing Case Type: Tricky Findings Explore more ways to learn on this and other topics by going to https://endlessmedical.academy/auth?h... QUESTION A 27-year-old man presents with 4 months of fluctuating proximal limb weakness, early fatigability when climbing stairs, and dry mouth. He notices transient strength improvement after brief vigorous efforts such as repeatedly rising from a squat. He has no diplopia at rest but reports intermittent blurred vision late in the day. He denies dysphagia. He lives alone, owns two cats, and reports daily marijuana use and heavy alcohol intake of 3-4 drinks per day.... OPTIONS A. Repetitive nerve stimulation at 20-50 Hz showing a postexercise compound muscle action potential increment of about 60-100%, indicating presynaptic Ca2+ channel dysfunction consistent with Lambert-Eaton myasthenic syndrome. B. Low-frequency (2-3 Hz) repetitive nerve stimulation demonstrating a greater than 10% decrement, supporting postsynaptic receptor impairment typical of myasthenia gravis rather than Lambert-Eaton myasthenic syndrome. C. Serum acetylcholine receptor-binding and blocking antibodies by ELISA, useful for generalized myasthenia gravis but not discriminatory for Lambert-Eaton myasthenic syndrome or botulism in this presentation; results do not change short-term electrodiagnostic interpretation. D. Bedside ice-pack test for ptosis improvement, a screening maneuver for ocular myasthenia that lacks specificity to distinguish Lambert-Eaton myasthenic syndrome from other neuromuscular junction disorders and offers no mechanistic localization to presynaptic dysfunction. CORRECT ANSWER A. Repetitive nerve stimulation at 20-50 Hz showing a postexercise compound muscle action potential increment of about 60-100%, indicating presynaptic Ca2+ channel dysfunction consistent with Lambert-Eaton myasthenic syndrome. EXPLANATION The correct answer is "Repetitive nerve stimulation at 20-50 Hz showing a postexercise compound muscle action potential increment of about 60-100%, indicating presynaptic Ca2+ channel dysfunction consistent with Lambert-Eaton myasthenic syndrome." This patient has proximal weakness, areflexia with postactivation facilitation, autonomic features (dry mouth), and transient improvement after brief maximal contraction, all typical of presynaptic neuromuscular transmission failure in Lambert-Eaton myasthenic syndrome. His electrophysiology already shows low baseline CMAPs with marked postexercise facilitation and large high-frequency increment, which is the most discriminating electrodiagnostic signature of presynaptic release failure.... Further reading: Links to sources are provided for optional further reading only. The questions and explanations are independently authored and do not reproduce or adapt any specific third-party text or content. --------------------------------------------------- Our cases and questions come from the https://EndlessMedical.Academy quiz engine - multi-model platform. Each question and explanation is forged by consensus between multiple top AI models (i.e. Open AI GPT, Claude, Grok, etc.), with automated web searches for the latest research and verified references. Calculations (e.g. eGFR, dosages) are checked via code execution to eliminate errors, and all references are reviewed by several AIs to minimize hallucinations. Important note: This material is entirely AI-generated and has not been verified by human experts; despite stringent consensus checks, perfect accuracy cannot be guaranteed. Exercise caution - always corroborate the content with trusted references or qualified professionals, and never apply information from this content to patient care or clinical decisions without independent verification. Clinicians already rely on AI and online tools - myself included - so treat this content as an additional focused aid, not a replacement for proper medical education. Visit https://endlessmedical.academy for more AI-supported resources and cases. This material can not be treated as medical advice. May contain errors. ---------------------------------------------------
Comments
-
 5 часов назад
5 часов назад
-
 3 месяца назад
3 месяца назад
-
 2 месяца назад
2 месяца назад
-
 9 месяцев назад
9 месяцев назад
-
 5 часов назад
5 часов назад
-
 1 месяц назад
1 месяц назад
-
 Трансляция закончилась 1 год назад
Трансляция закончилась 1 год назад
-
 2 месяца назад
2 месяца назад
-
 10 дней назад
10 дней назад
-
 2 часа назад
2 часа назад
-
 1 месяц назад
1 месяц назад
-
 10 месяцев назад
10 месяцев назад
-
 1 день назад
1 день назад
-
 2 месяца назад
2 месяца назад
-
 11 минут назад
11 минут назад
-
 3 месяца назад
3 месяца назад
-
 3 недели назад
3 недели назад
-
 5 часов назад
5 часов назад
-
 7 дней назад
7 дней назад
-
 2 часа назад
2 часа назад